
Written by Dr. Dennis Hartlieb
Canted Smile Guide:
7 Reasons for the Unaesthetic Canted Smile and What Cosmetic Dentists Can Do to Treat Them
When your patient presents with a canted smile, your goal is to find the underlying cause of misalignment and create a treatment plan targets the root of the problem. This blog examines potential causes of the canted smile and conservative treatment options available.

What Causes a Canted Smile?
7 Factors That Can Contribute to Unaesthetic Canted Smiles
Considering Smiles: A Little Background About Me

On this particular week that Donny had abandoned me, I was feeling a bit grumpy about the unfair twist that life had dealt me. My buddy was gone, my older siblings treated me like a parasite, my parents also had no time for 9-year-old me, as they were busy living the life of those who have to raise a family and make a living… but there was Ted.
Ted was an elderly neighbor who lived across the street. I suspect he was probably in his sixties, having retired from his career working for one of the ‘Big 3’ automotive factories (General Motors, Ford and Chrysler).
Ted was sitting on his front porch, a one-story suburban ranch with aluminum siding – classic 1950s Americana, with white trim and faux black shutters. The lawn was flat and finely manicured - the product of civic pride and a boat-load of time to do one’s part to keep the neighborhood clean and respectable.
Ted’s house had a one-car, detached garage. It was painted white to match the house. The garage door was a one-piece door that opened and closed all as one. As it turns out, this simple white, suburban garage door would serve perfectly as a canvas for Den and Ted’s most excellent adventure!
Ted decided that this week would be a good week to paint his garage door. So Ted said to me, “Den, how about we paint a big smiley face on the garage?”
Ted was an elderly neighbor who lived across the street. I suspect he was probably in his sixties, having retired from his career working for one of the ‘Big 3’ automotive factories (General Motors, Ford and Chrysler).
Ted was sitting on his front porch, a one-story suburban ranch with aluminum siding – classic 1950s Americana, with white trim and faux black shutters. The lawn was flat and finely manicured - the product of civic pride and a boat-load of time to do one’s part to keep the neighborhood clean and respectable.
Ted’s house had a one-car, detached garage. It was painted white to match the house. The garage door was a one-piece door that opened and closed all as one. As it turns out, this simple white, suburban garage door would serve perfectly as a canvas for Den and Ted’s most excellent adventure!
Ted decided that this week would be a good week to paint his garage door. So Ted said to me, “Den, how about we paint a big smiley face on the garage?”

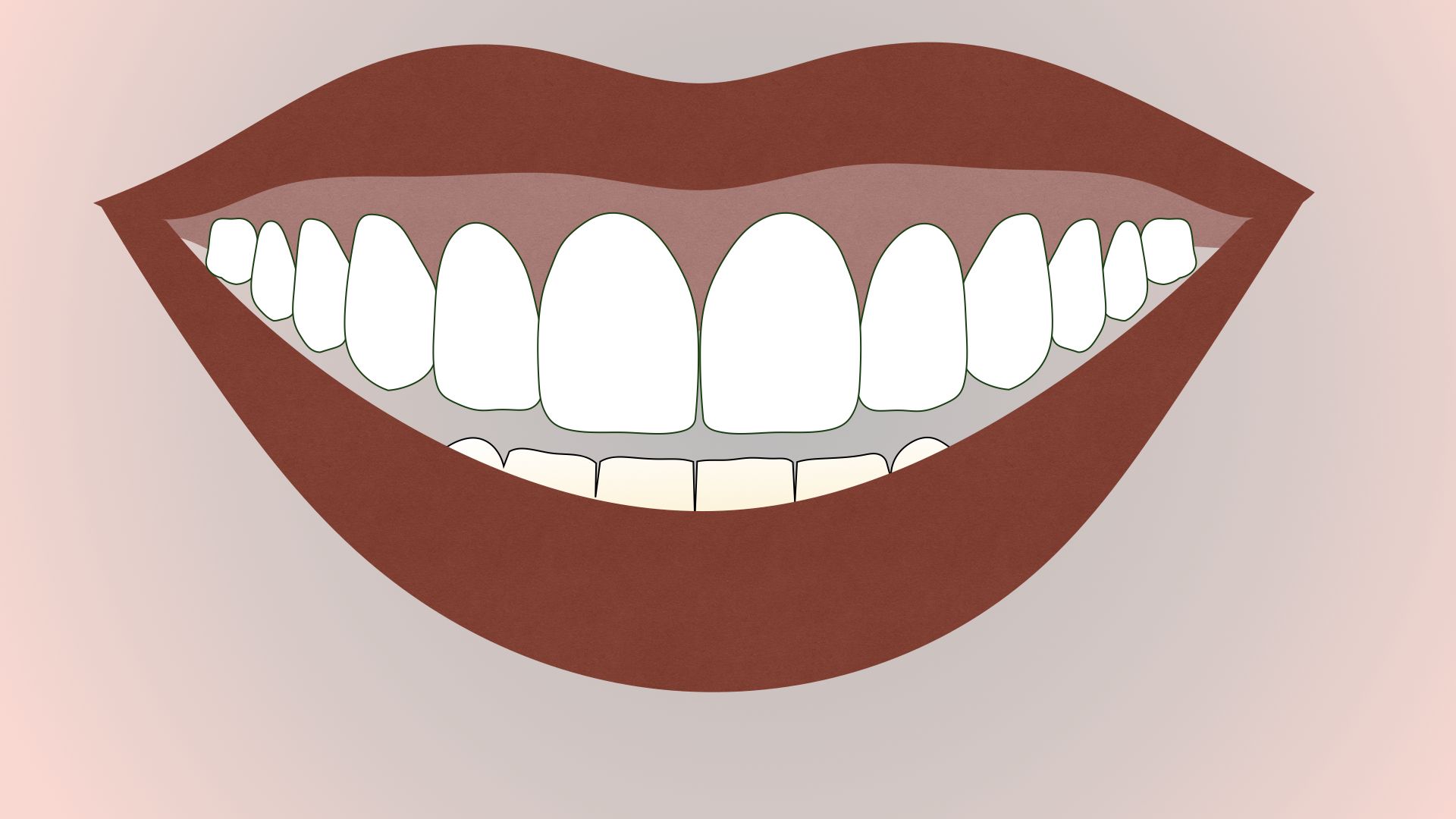
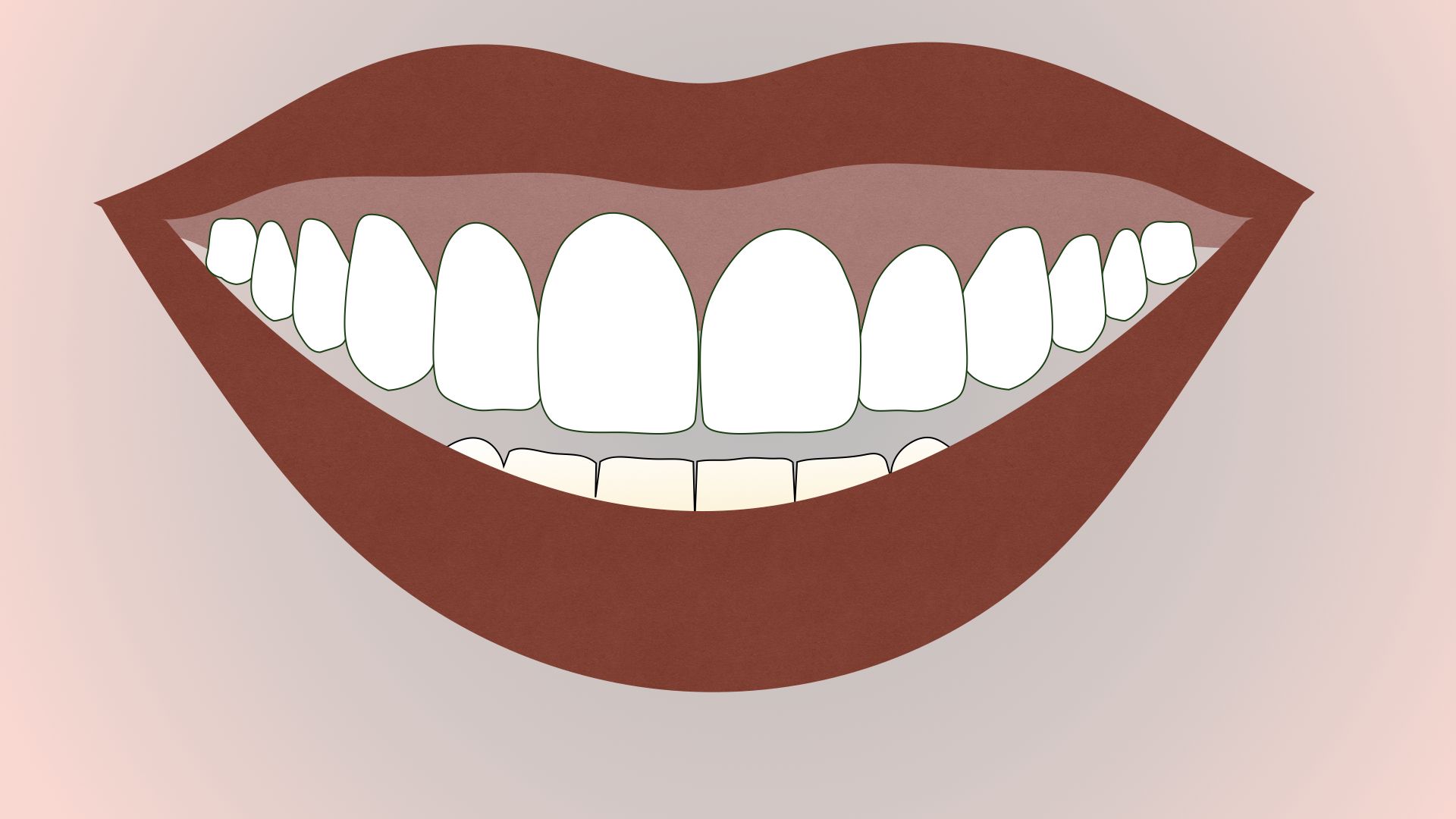
Canted Smile: A canted or crooked smile refers to a smile that is not level across the horizontal plane of the face. It is a smile that is tilted or slanted.
Seven Factors Contributing to Canted Smiles
Medical Considerations
Kevin L. Hicks, DDS
DOT Premium Member, Survey Response
Lip Asymmetry


Pro tip: Before and After photos can support you as the clinician in many ways, including instances where patients believe that your dentistry caused a dental problem.
Antonela Schroeder, DMD
DOT Premium Member, Survey Response
Gummy Smile


Alloderm: A dermal matrix derived from human donor tissue that can be used for gum grafting.
Option #3
Uneven Wear on Teeth

Deborah Fung, DDS, MAGD
DOT Premium Member, Survey Response
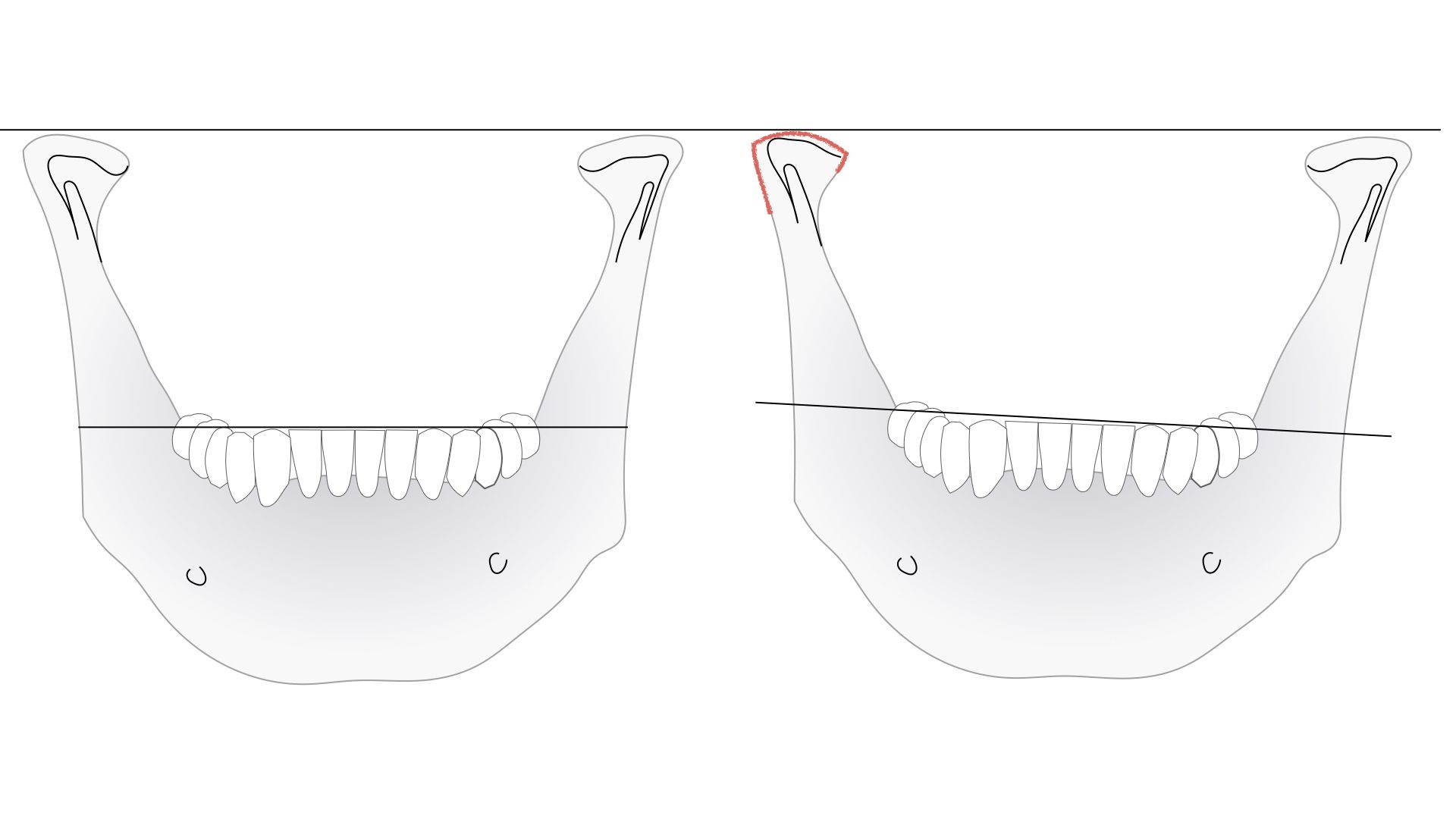
Missing or Undersized Teeth
If posterior (back) lower teeth are missing, the upper back teeth will erupt (move downward) due to the lack of occlusal (bite) stability. As the upper teeth erupt, the gum tissue, which is attached to the teeth, will also erupt resulting in a canted, or crooked, smile.

The Ultimate Finishing and Polishing Guide for Anterior Composite Restorations

Poor Occlusion / Bad Bites



TM Joint Issues

Final Thoughts about Canted Smiles
Dennis Hartlieb, DDS, AAACD
Share this page
Thank you!
Latest from our blog
