
A Guide to Assessing and Treating the Anterior Open Bite

Unilateral cross-bites, bilateral cross-bites, deep bites, super-erupted teeth, roller-coaster bites…these are the dental and skeletal orthodontic cases that we all learned about while in dental school.
While there will be discussion, and even arguments, over the appropriate treatment for any of these types of dental malocclusions, there is another malocclusion that we see commonly in our dental practices that I did not learn about in my dental education that had me stumped during my early years in dentistry – the anterior open bite.
Malocclusion. This word to most dentists will invoke a variety of thoughts and visual scenarios. From the Class II bite (pic 1) with the retrognathic mandible to the Class III end-to-end occlusion (pic 2).
What is an Anterior Open Bite?
What is an Anterior Open Bite?
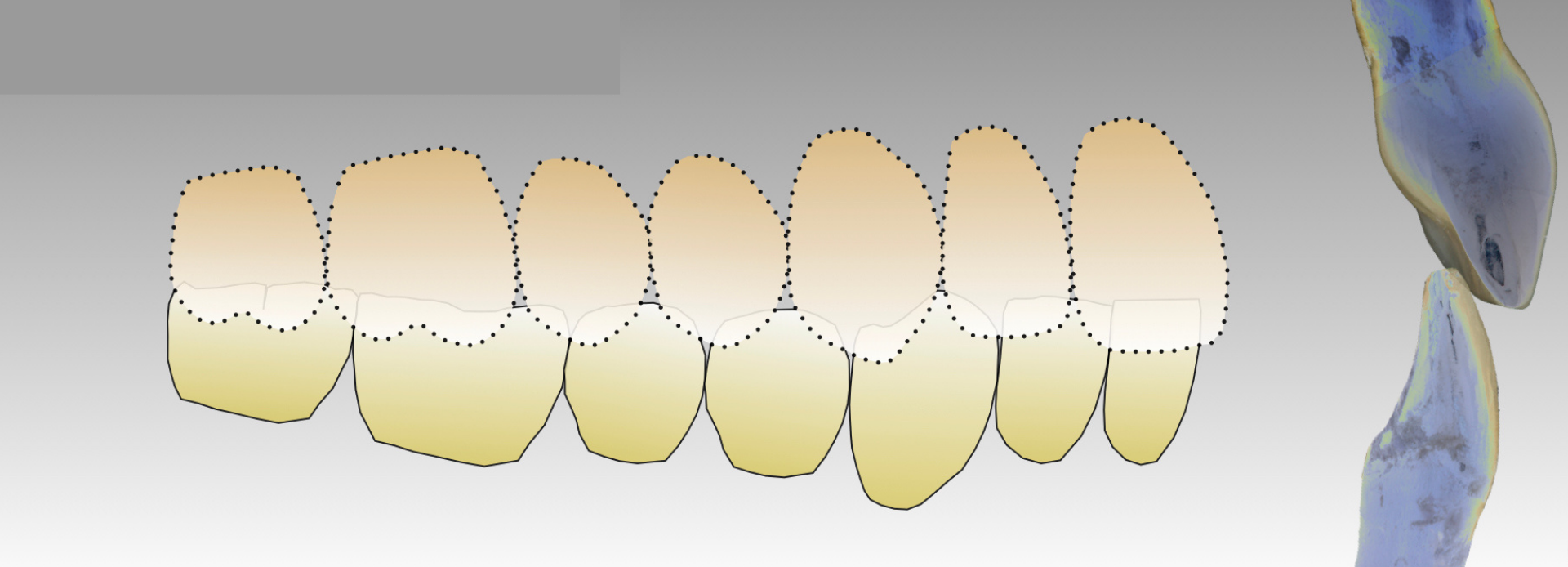
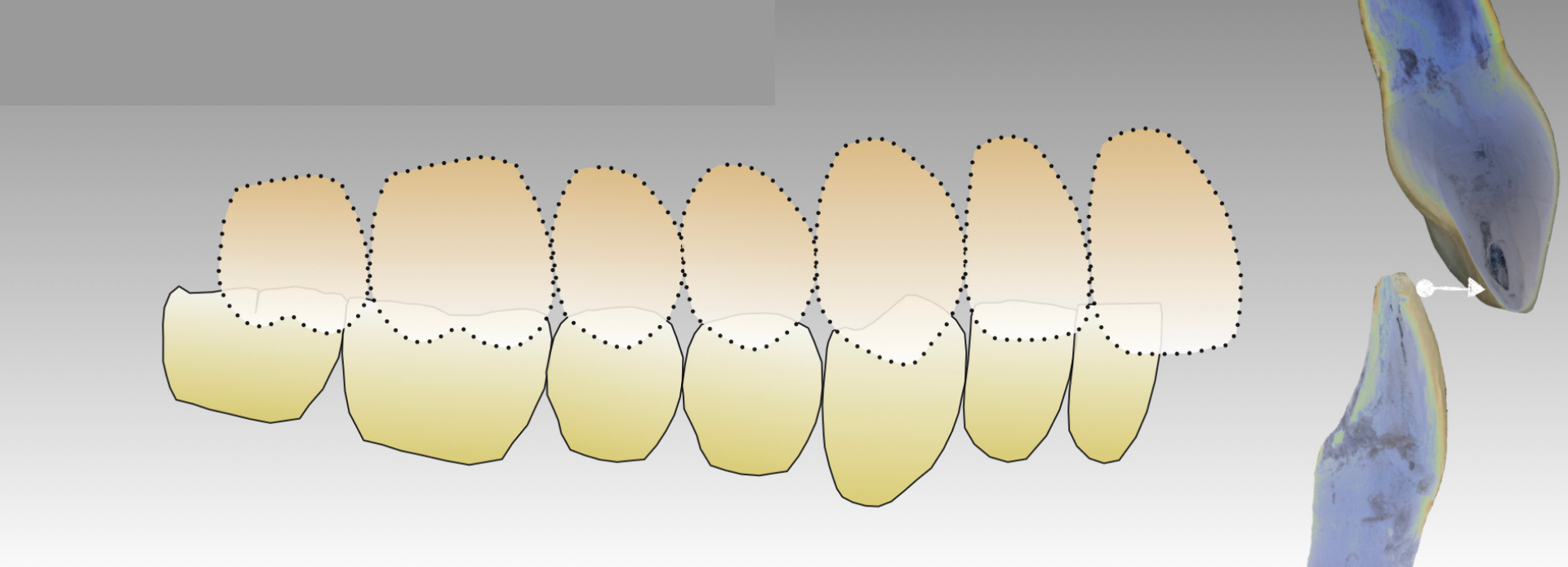
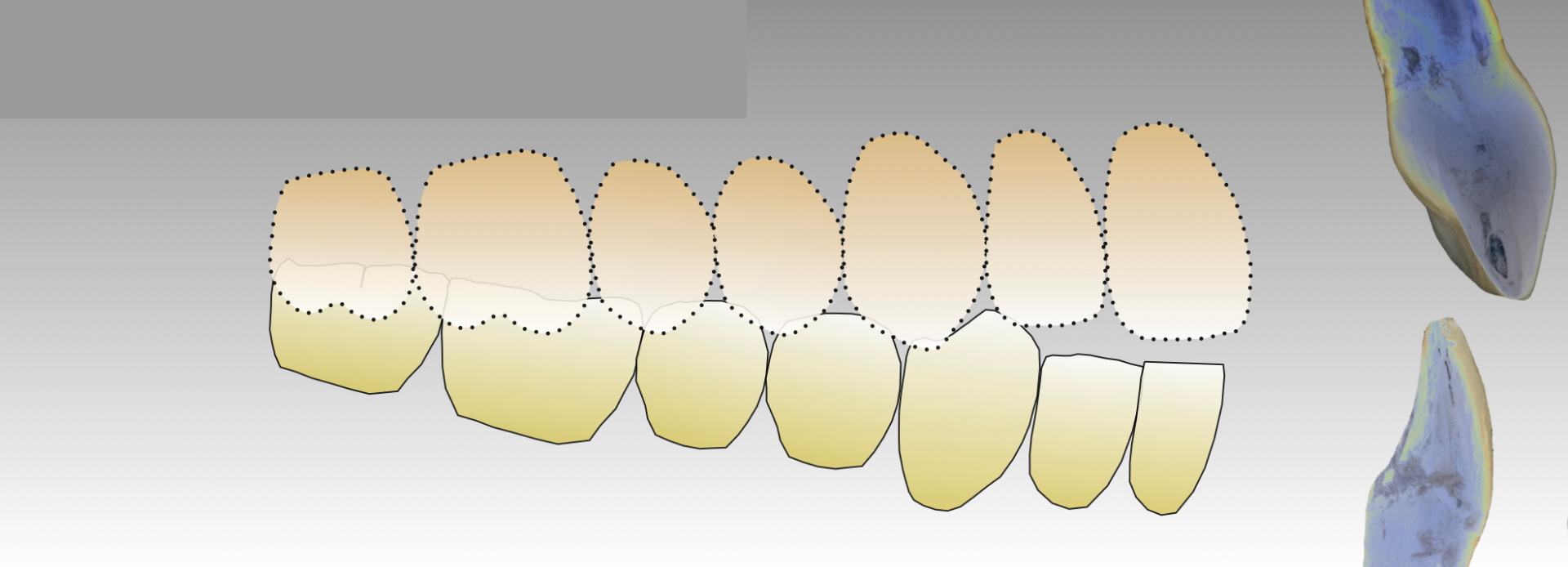
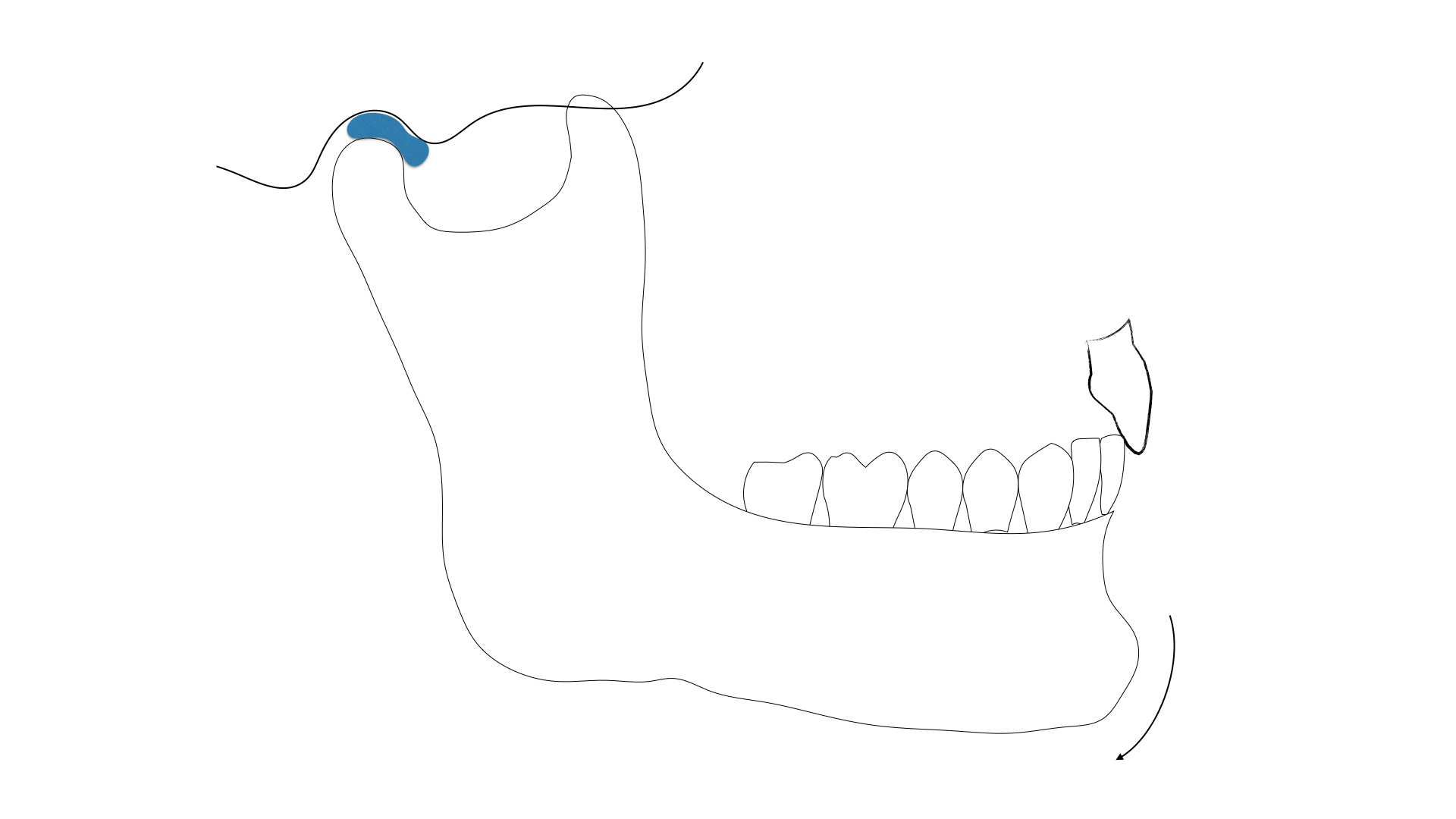
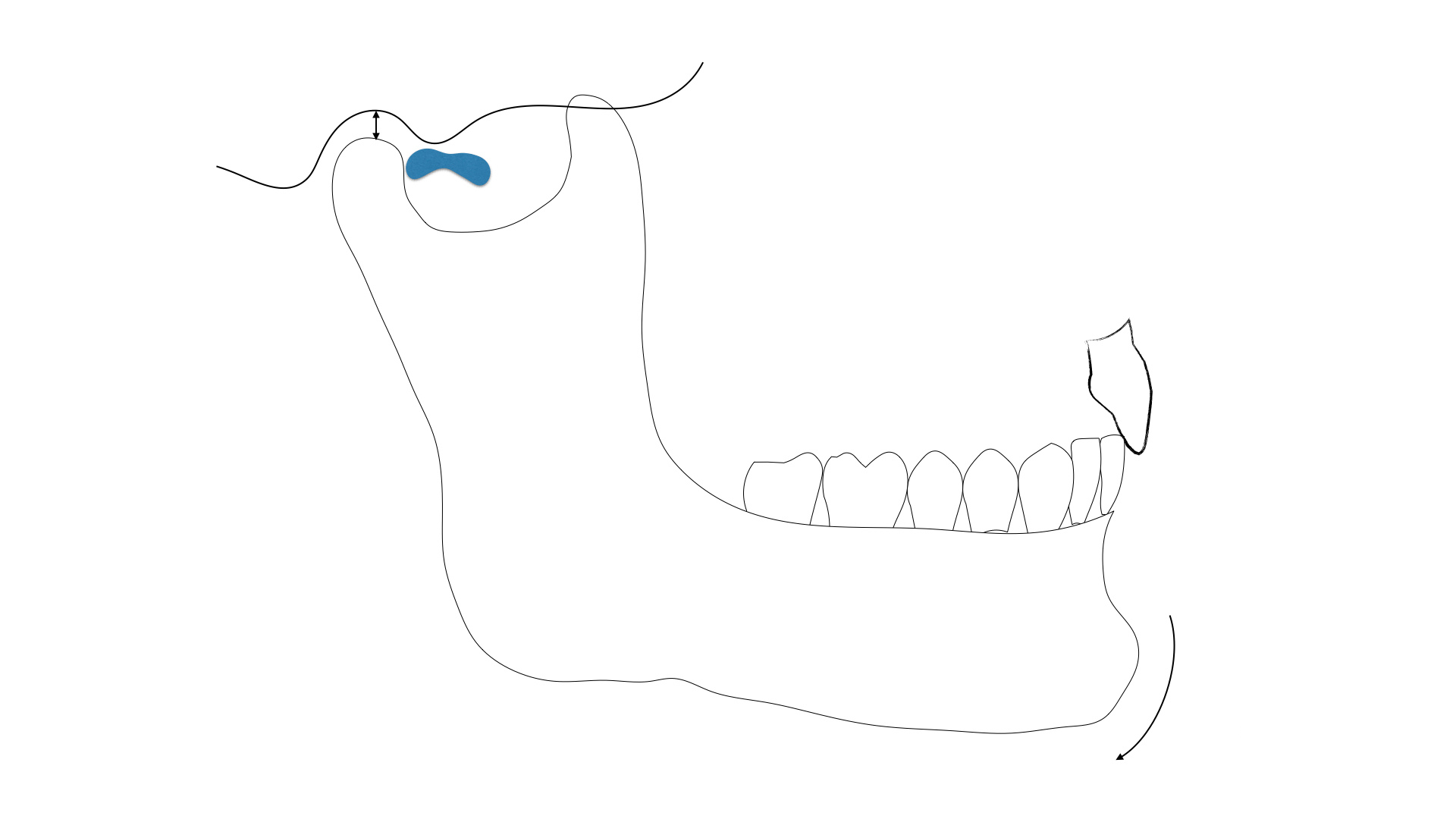
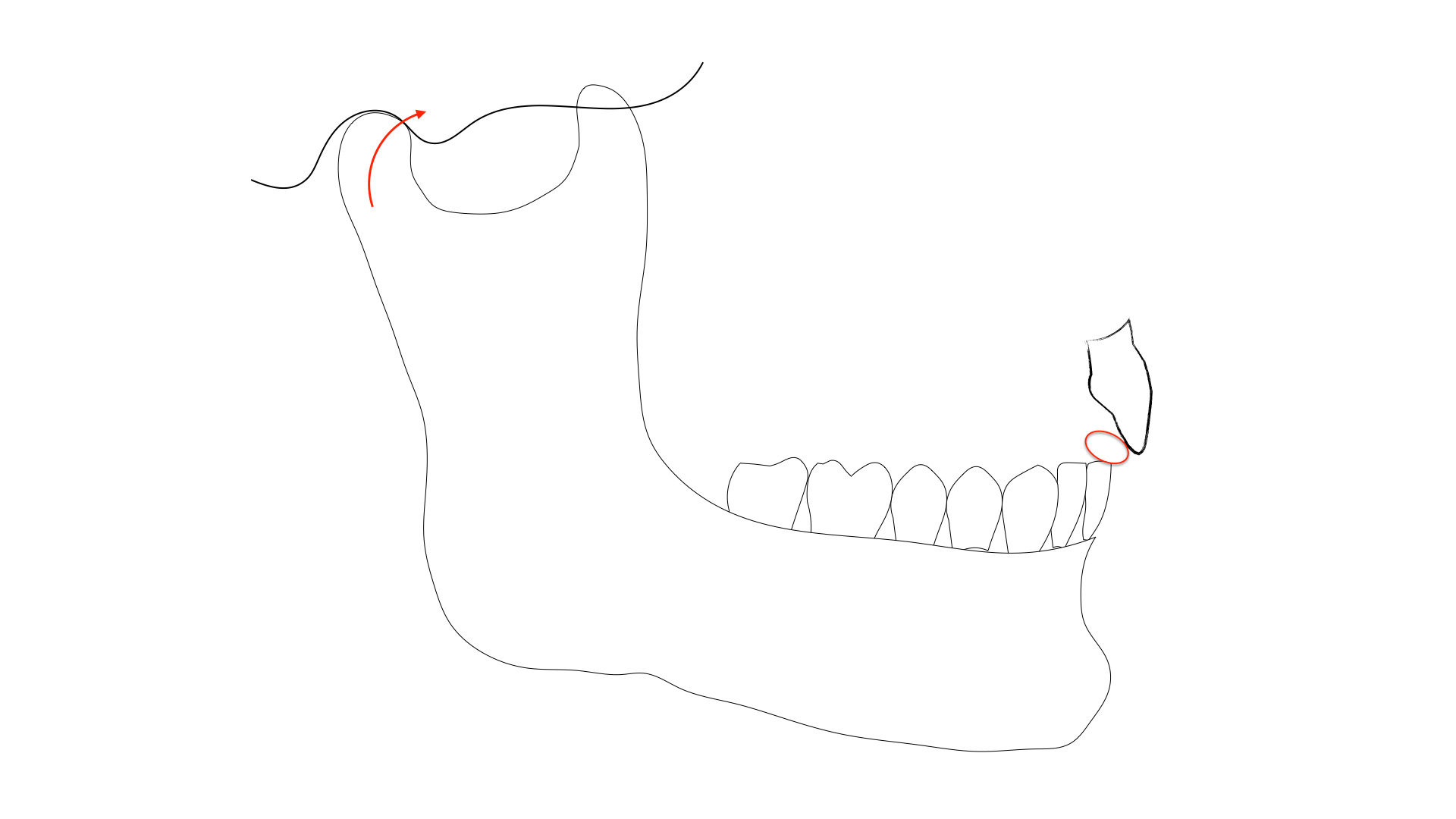
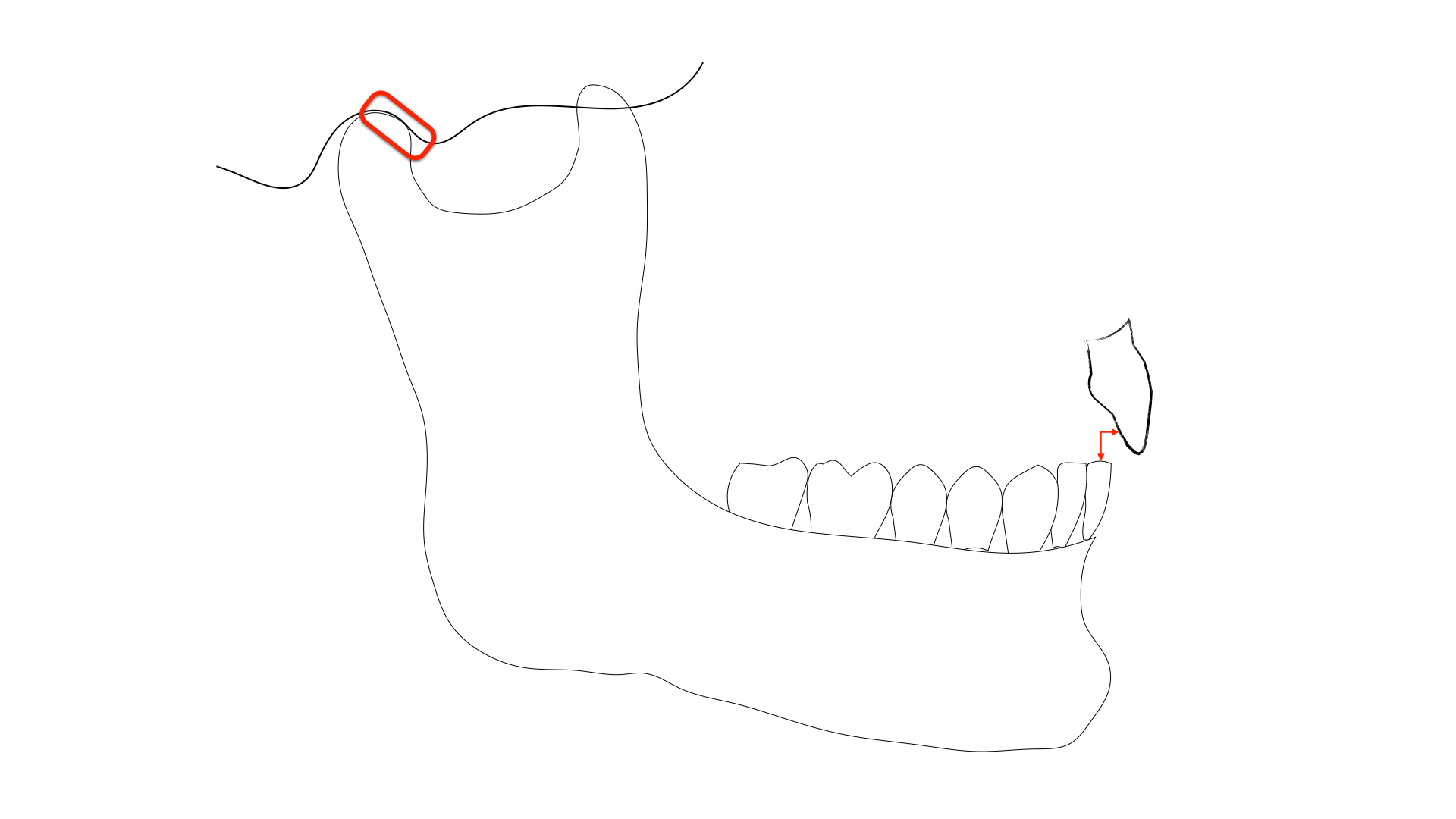
While anterior open bite cases can also be Class II malocclusions, these cases differ from the classic Class II cases because not only is there a horizontal discrepancy between the maxillary anterior teeth and mandibular anterior teeth, but there is also a vertical gap (see illustration 1, 2, 3).
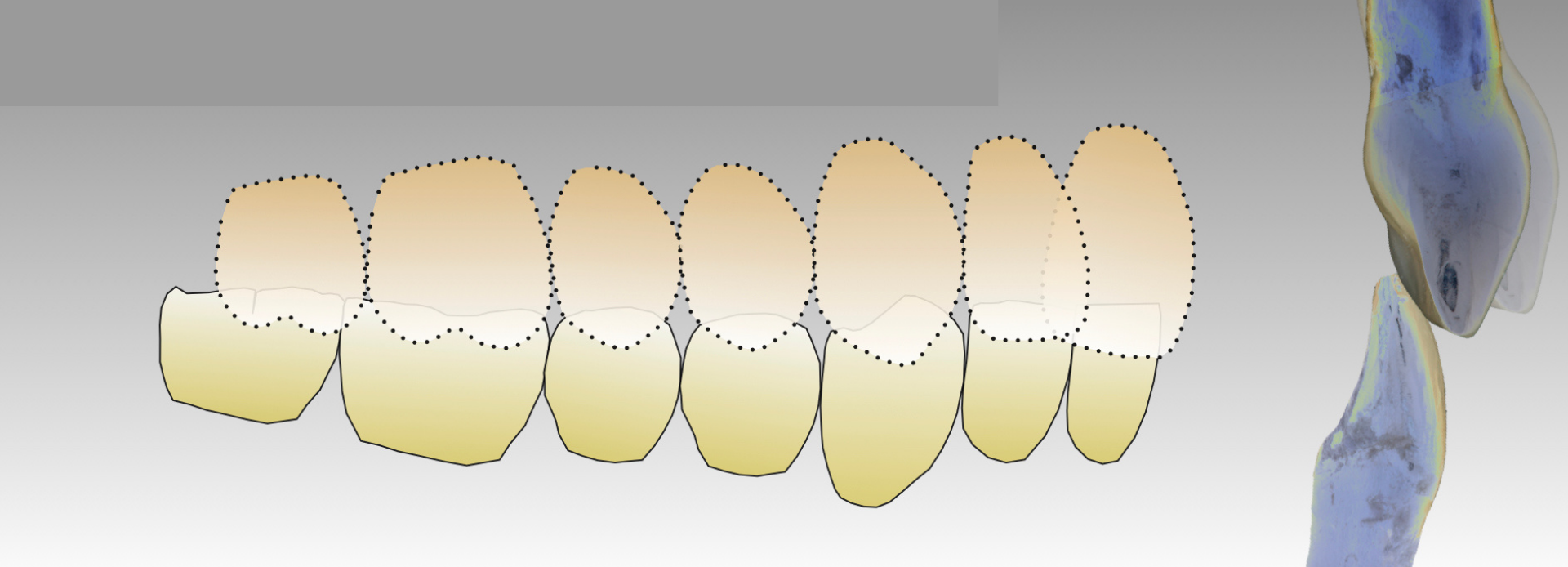
In fact, in a Class II, division II case, there is commonly contact with the maxillary and mandibular incisors as the central incisors have become palatally tipped (illustration 4). So, indeed, anterior open bites can be in any occlusal relationship – Class I’s, Class II’s, and Class III’s.
So, over the years, I’ve been wondering - why with some patients do we see a gap between the upper and lower front teeth? We’re taught that teeth are supposed to erupt until they come in contact with an opposing tooth, and in the anterior dentition, if the bite is not stable, the teeth will over-erupt, or super-erupt creating a deep bite. So why aren’t the front teeth coming together with these anterior open bites?
Correcting these anterior open bites can be challenging for the orthodontist. Try as they may, some of the open bites just don’t seem to want to close. Orthodontists I have worked with would typically consider that the patient has a strong tongue thrust, or forward tongue posturing habit, that would prevent the closing of these open bites with orthodontics.
What Causes the Anterior Open Bite?
When teeth and muscles battle, muscle wins.
- Peter Dawson, DDS
Can we Correct the Anterior Open Bite?
Temporomandibular Joint & the Anterior Open Bite
After evaluating a tremendous number of MRI’s of patients with anterior open bites, they all, yes all, have displaced discs.
RANDY VALENTA, DDS
DOT Premium Member, Survey Response
Orthodontic Treatment of the Anterior Open Bite

Airway & the Anterior Open Bite
DOT Premium Member, Survey Response
DARREN G. KOCH, DDS
DOT Premium Member, Survey Response
Tongue-Tie & the Anterior Open Bite

Anterior Open Bite Patient Evaluation Checklist:
Survey Results
Survey Results
If the anterior open bite patient has no joint pain, and no esthetic or functional concerns, which best describes your first course of action?




If the anterior open bite patient HAS TM joint pain, which would likely be your treatment recommendation:





If the patient HAS NO TM joint pain but is dissatisfied with the appearance of their smile, which of the following would you include in your treatment recommendations?





The patient in the photograph has two bites, an MIP where all the teeth fit together and a seated joint position bite where only posterior teeth touch.
If the patient has no TM joint pain, what would be your likely first recommendation to the patient?

If the patient does have TM joint pain, what would be your likely first recommendation to the patient?



Final Thoughts...
Final Thoughts...
Dennis B. Hartlieb, DDS, AAACD
Share this page
Thank you!
Latest from our blog
