
DR. DENNIS HARTLIEB

Bounce Back! Are Dentists Using Rubber Dam Isolation in Practice?
Do you use a rubber dam in your practice? Rubber dams have their advantages and disadvantages as a dental tool. Take a look at what cases I typically elect to use a rubber dam, and find out what the DOT community has to say about rubber dam usage in the dental practice.
Drag to resize
(Read time 5-7 minutes)

How long have dentists been using rubber dam?
So, after doing some research (hello Google), it turns out that dentists have been using rubber dams for over 150 years. Now, there are days in the practice that my back feels like I’ve been in practice that long, but I’m shocked that the rubber dam has been around for over a century.
I’m not sure about your dental school experience, but at the University of Michigan School of Dentistry, it seemed like all restorative procedures were done with rubber dam. In fact, I remember quite well personally being ‘rubber-dammed’ for a gold onlay try-in and cementation that took 3 hours back when I was a second-year dental student.
I’m not sure about your dental school experience, but at the University of Michigan School of Dentistry, it seemed like all restorative procedures were done with rubber dam. In fact, I remember quite well personally being ‘rubber-dammed’ for a gold onlay try-in and cementation that took 3 hours back when I was a second-year dental student.
Drag to resize
Three Things that I Prefer not to Talk About in Public Venues:
Drag to resize

Now, if you’re like me, the minute you got out of dental school, you stopped using a rubber dam (I did use them for the short period of time that I did root canals). I don’t know why I immediately stopped using the rubber dam... maybe I didn’t want to spend the extra time for the restorative procedure (funny enough, my practice was mighty slow so that would not have been a good reason!), maybe I thought that I was doing my patients a favor by not subjecting them to this medieval torture device, maybe I was just plain lazy. Regardless of the reason, or reasons, I have over the past decade come to embrace the rubber dam, this, my little elastic mistress.
I have learned that there are three things that I prefer not to talk about in public venues; politics, religion, and rubber dam usage
(though some could argue that rubber dam usage is kind of a religion for some). As many of our readers experienced, dentists can be quite opinionated on rubber dam usage. Case in point, Colin Pop wrote recently in his excellent rubber dam isolation article from the Journal of Cosmetic Dentistry, “the use of rubber dam isolation is a precaution that should always be followed during dental procedures.” Always. Many of our readers will agree with this sentiment. I was raised with the belief that we should never say always, and with rubber dam usage, I strongly agree.
Drag to resize
Advantages of Using the Rubber Dam
I believe that there are other excellent opportunities for isolation available in dentistry today. I also do not think that you should be shamed if you choose not to use a rubber dam for your restorative treatment. And to be clear, I don’t use rubber dam isolation for all of my restorative procedures. I have come to love the rubber dam for posterior direct restorations and for onlay cementations.
But when it comes to anterior restorative treatment, I use a variety of isolation methods. I do pull out the rubber dam when I’m treating the ‘grunge’ mouth and fighting to keep the tooth/teeth from bleeding gums, or for other isolation reasons. Basically, here are, in my opinion, some of the advantages of using the rubber dam:
But when it comes to anterior restorative treatment, I use a variety of isolation methods. I do pull out the rubber dam when I’m treating the ‘grunge’ mouth and fighting to keep the tooth/teeth from bleeding gums, or for other isolation reasons. Basically, here are, in my opinion, some of the advantages of using the rubber dam:
1. Moisture Control
Using a rubber dam does not guarantee absolute moisture control. Seepage can occur when using a rubber dam, but for the most part, I can keep the teeth that I’m working on pretty darn dry when using a properly positioned rubber dam. Choosing the correct clamp and ligating teeth with floss are important to minimize leakage of the rubber dam (picture 1 and 2).
(Left to right) Picture 1, Picture 2
2. Visibility
I know dentists that use the rubber dam because it can give a really nice visual contrast for dental photography. I think that’s fine, but that isn’t the visibility that I’m referencing. The contrasting color of the rubber dam actually is beneficial when doing restorative dentistry.
For me, it’s visually easier when I’m working in the proximal box and along the cervical floor to differentiate healthy tooth structure from caries, and to retract gingival tissue in Class V and Class III composites (picture 3).
For me, it’s visually easier when I’m working in the proximal box and along the cervical floor to differentiate healthy tooth structure from caries, and to retract gingival tissue in Class V and Class III composites (picture 3).

Picture 3
3. Protection
Both for the patient and for the dental team! A pediatric dentist colleague of mine describes the rubber dam as a ‘seat-belt’ to her patients and parents. The rubber dam prevents aspiration of materials when working in the mouth. The use of a rubber dam during aerosol producing procedures can help limit the risk of exposure to viruses, putting patients, dentists, and staff at lower risk of infection.
4. Adhesive Predictability
The research on dentin adhesion is clear – saliva, blood, and other oral contaminates can lessen the potential of our adhesive bond during restorative dental procedures.
Case in point - I was right in the middle of cementing a couple of eMax onlays when my patient started hacking during the procedure (we’ve all been there) – with the rubber dam in place the teeth remained isolated and we were able to continue the procedure without contamination.
Interestingly, this patient was not happy when we were placing the rubber dam, but afterwards when I explained that if we had not been using the dam, the quality of the bonding would have absolutely been violated without it, she was understanding of the extra attention for her benefit (plus, it kept her from hacking all over me and my dental assistant!).
Interestingly, this patient was not happy when we were placing the rubber dam, but afterwards when I explained that if we had not been using the dam, the quality of the bonding would have absolutely been violated without it, she was understanding of the extra attention for her benefit (plus, it kept her from hacking all over me and my dental assistant!).
Picture 4
Drag to resize
Survey: What the DOT Community has to say
We surveyed some of our top Dental Online Trainers about rubber dam usage in the dental practice. Some of their responses are included below. Special thank you to participants of this survey for your contribution to DOT.
The following are a couple of questions we asked our focus group about rubber dam usage and other techniques for isolation:
The following are a couple of questions we asked our focus group about rubber dam usage and other techniques for isolation:
I was not surprised to learn that many of our DOT members use rubber dam routinely for isolation. Our participants included comments like, "Rubber dams are awesome!," and "Learn how to efficiently use rubber dams as early as you can in your career and continue to use them."
I think this last comment is a great point. I’ve spoken to many dentists that simply say that they are out of the habit of using the rubber dam (since dental school) and it’s difficult to slow down the office to relearn placement techniques. I couldn’t agree more and understand this issue very well. To help those who want to get back in the rubber dam habit and become a ‘Rubber dam fan’ I’ll give some recommendations and tips at the conclusion of this blog.
The bottom line on rubber dam usage according to our survey
-
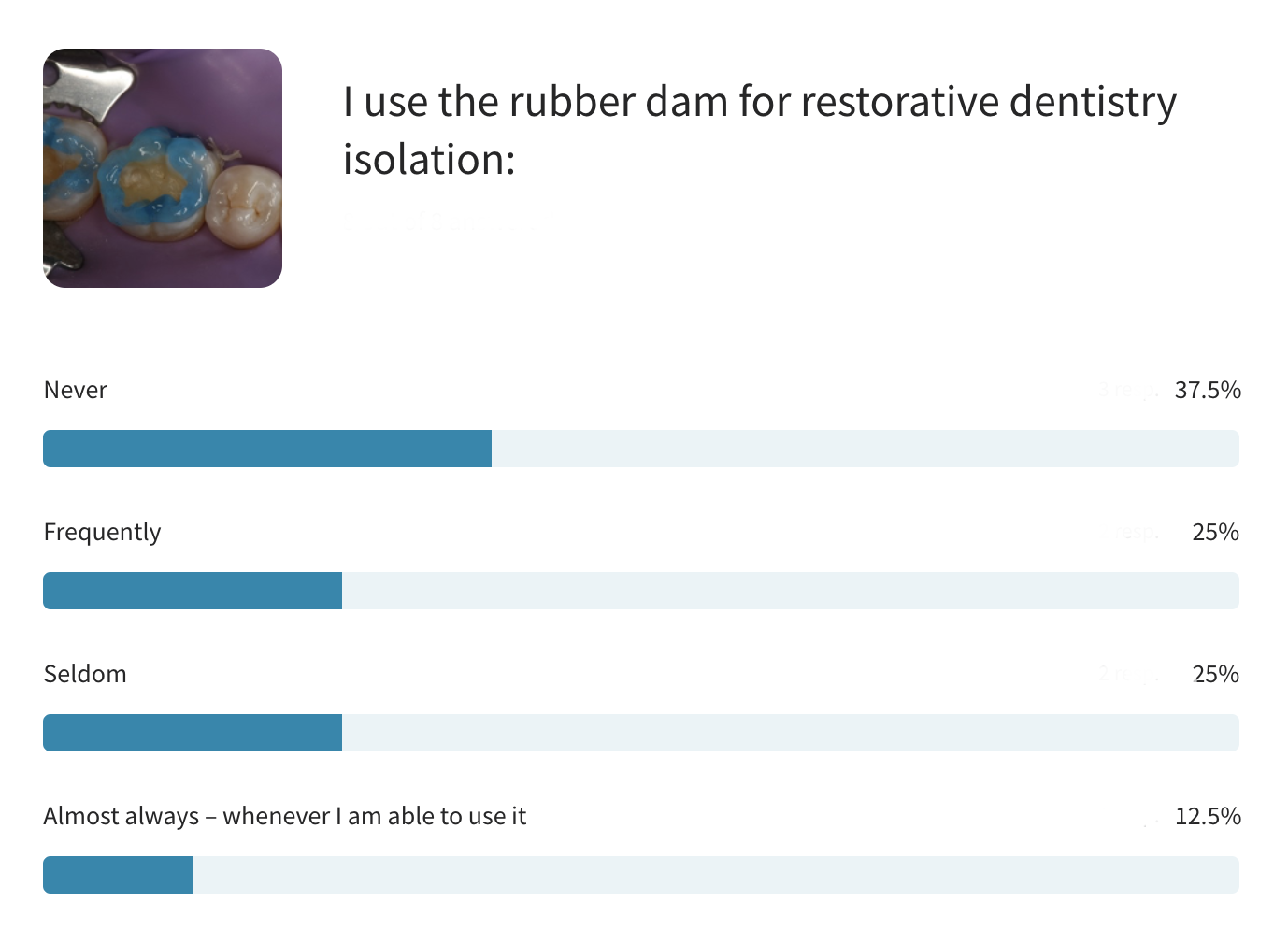
Over 60% of dentists use rubber dams within their practice
-
33% of dentists say they use rubber dams frequently or almost always
-
40% of dentists shared that they never use a rubber dam for restorative dentistry isolation
The main reasons for the lack of rubber dam use included: 1) being out of habit (as mentioned above), 2)
that their patients did not like using the rubber dam, or 3) they had
other techniques or systems for isolation during procedures.
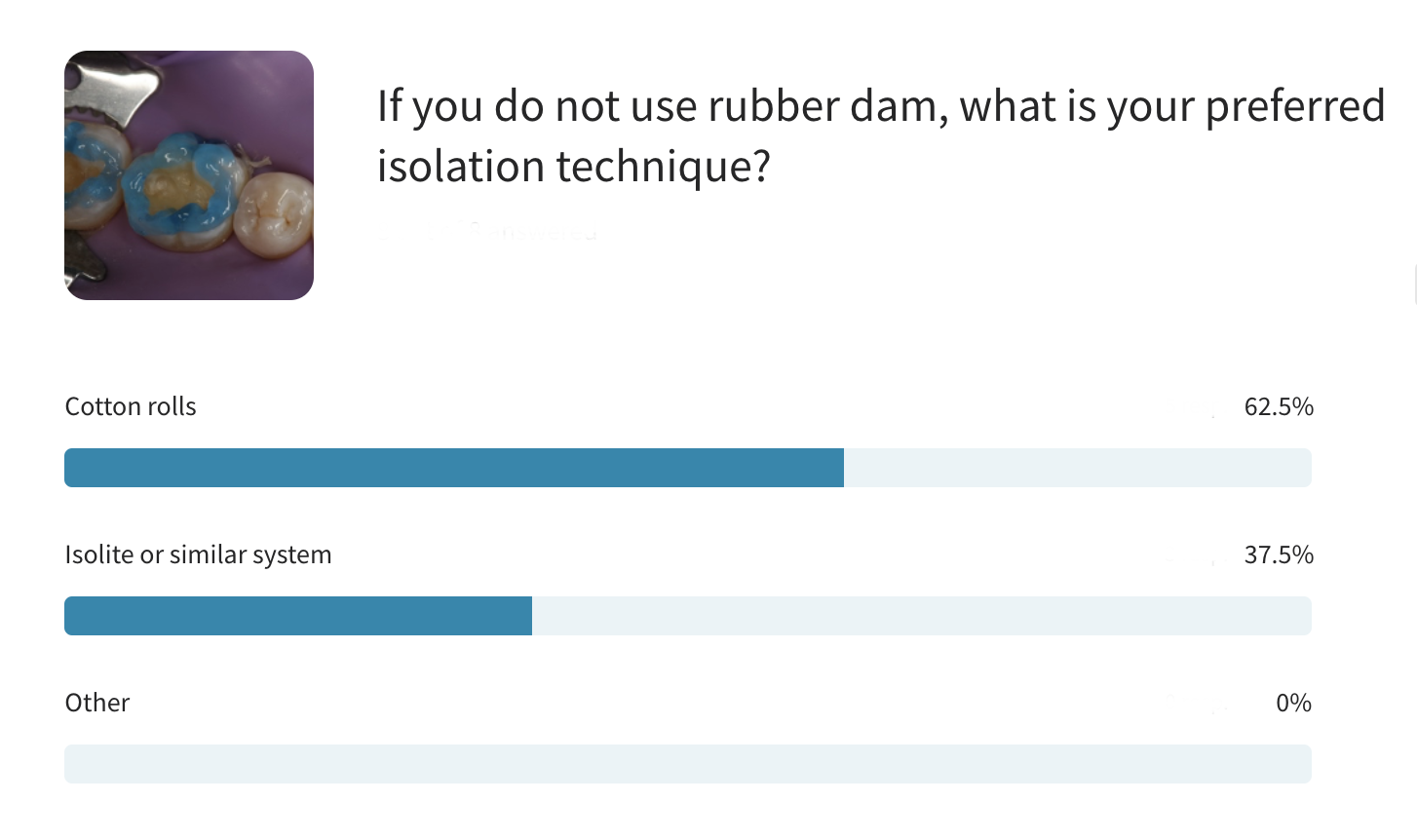
Surveyed members stated “I will use OptraGate for anterior restorations, and it tends to work well for isolation."
I also use the OptraGate regularly in my practice as well. In the following section of this blog, Isolite and cotton rolls were also mentioned as techniques used in practice to maintain isolation during restorative procedures.
My thoughts on alternative isolation methods
1. OptraGates
OptraGate (picture 5), from Ivoclar Vivadent, comes in several sizes (regular, small and junior) and colors (white, blue and pink). The OptraGate is a wonderful tool for pulling the lips away from the operatory field. It is simple and efficient to use, and most patients are comfortable with the OptraGate in place.
I have found that the plastic frame of the OptraGate can rub against the sensitive mucosal and gingival tissues, so we will often place a small portion of a 2x2 gauze under the front portion of the frame to create a cushion and improve comfort for our patients.
I have found that the plastic frame of the OptraGate can rub against the sensitive mucosal and gingival tissues, so we will often place a small portion of a 2x2 gauze under the front portion of the frame to create a cushion and improve comfort for our patients.
Write your awesome label here.
Picture 5
We use the OptraGate in our practice for multiple procedures including:
-
In-office bleaching
-
Anterior direct resin bonding
-
Icon white spot removal treatments
-
Intraoral scanning
-
Class V restorations
for bicuspids -
Placement/Cementation of porcelain veneers
-
Smile Preview/Trial Smile appointments
As you can see in the image above, the OptraGate really pulls the lips away from the treatment area. Additional isolation methods may be necessary when using the OptraGate. When doing in-office bleaching, or when using Icon, we will use a liquid rubber dam material to protect the gingival tissues. For direct resin bonding techniques, I will typically place retraction cord to reduce influence of sulcular fluids during the restorative procedure.
2. Isolite
I’ve had the Isolite in my practice since I first saw it presented at the Chicago Midwinter Meeting many, many years ago. For those not familiar, the Isolite (now part of the Zyris system of Isolite/Isodry) - is a disposable bite block and svedopter all-in-one. It is described as an “all-in-one continuous evacuation, tongue retraction, airway protection and illumination system.
Isolite (picture 6) is great for:
Isolite (picture 6) is great for:
-
Patients with heavy saliva flow
-
Quadrant dentistry, and when I’m working on those challenging distal upper molars
-
Managing aerosols and keeping the tongue away from the drill and restorative area when we’re doing our dentistry
-
Placing sealants – it keeps the teeth to be worked on absolutely dry without having to anesthetize the patient for rubber dam placement.
The Isolite is a mouthful - I do find that some patients are challenged with the size and bulkiness of the Isolite, and personally, the noise from the suction can be hard on my ears… I feel like I’m sitting outside a jet engine. If you have not worked with the Isolite before, click here to get more information.
Write your awesome label here.
Picture 6
3. Cotton Rolls & Dry Angles
When not using a rubber dam or OptraGate, cotton rolls and dry angles can act as a suitable isolator. Cotton rolls and dry angles are the work horse in most dental practices for routine restorative procedures.
Using these cotton barriers to block the parotid gland ducts in the cheeks and the saliva glands in the floor of the mouth, you'll typically be able to find an adequately dry work area. I use cotton rolls and dry angles routinely for uncomplicated restorative procedures on patients that I don’t feel the need to use more complicated methods for isolation (i.e. rubber dam).
Using these cotton barriers to block the parotid gland ducts in the cheeks and the saliva glands in the floor of the mouth, you'll typically be able to find an adequately dry work area. I use cotton rolls and dry angles routinely for uncomplicated restorative procedures on patients that I don’t feel the need to use more complicated methods for isolation (i.e. rubber dam).
Drag to resize
Rubber Dam Usage and Patient Comfort
As I stated in the beginning of this blog, I was reluctant to use rubber dams in practice. I thought that the rubber dam was too uncomfortable for patients and that it would negatively affect my practice (scare patients away). Here is what I think now:
-
Many patients actually like and prefer their dental treatment with the rubber dam
-
In many cases, it makes my dentistry easier
-
My photographs for teaching are cleaner and better for presentation (picture 7) - check out this dental photography course by Dr. Chris Ching
-
My dentistry is often better with the use of the rubber dam – especially porcelain onlay preparation and cementation (picture 8)
-
Shockingly (for me), it has been a practice builder

Picture 7

Picture 8
Drag to resize
This last point is important to review – it has added value to my practice. The rubber dam can be part of helping patients understand your commitment to excellent dentistry. It is unlikely that your patient has experienced other providers using a rubber dam, so it is important that the advantages of the rubber dam is ‘sold’ to the patient before using.
I was taught by Walter Hailey, a dental consultant from years past that patients dial into WIIFM – What’s In It For Me. So, when you talk about the advantages, don’t talk about the fact that it protects you and your dental team from possible infectious diseases from the patient.
I was taught by Walter Hailey, a dental consultant from years past that patients dial into WIIFM – What’s In It For Me. So, when you talk about the advantages, don’t talk about the fact that it protects you and your dental team from possible infectious diseases from the patient.
Talk to the patient about how the dentistry will be better. How the materials that we use are very susceptible to moisture and if we keep the tooth absolutely dry during treatment, the dentistry should last longer.
I also tell patients that we are removing amalgam restorations, that the rubber dam will keep the mercury from the amalgam out of their mouth so that there is less risk to them as we replace their restoration (picture 9). WIIFM – remember that when talking to your patients – it’s the things that we do to make our dentistry different, and better, for the patient.

Picture 9
Drag to resize
5 Tips for Rubber Dam Usage and Patient Comfortability
- Patient Education - There are patients that say that they can’t breathe through their nose – those patients need to be assured that there is enough space around the rubber dam that they can adequately breathe. In fact, it is better than when we are stuffing them with cotton and suction devices. They don’t have to worry about inhaling any by-products from the drilling with the rubber dam in place.
- Take baby steps - Start with a lower first molar occlusal composite. You only need to punch one hole in the rubber dam. No need to use floss ligatures. Easy peazy.
- Make sure your patient is numb – it can be a challenge to give an additional mandibular block with a rubber dam in place
- For upper teeth, I place topical anesthetic on the palatal tissue so that patients don’t feel the pinch of the clamp
- I like to place the clamp first, then place the rubber dam over the clamp. I always ligate the clamp if it is going on before the rubber dam to prevent aspiration of the clamp. 100% of the time.
Rubber dams can save your practice from a potential lawsuit if the patient inhales materials, instruments, or irritants during a procedure.
Drag to resize
Remember, we are responsible for the patient's overall care as a dentist. One of the main components of the rubber dam is the protection of the GI tract and airway. If you are doing root canals in your practice it's essential to isolate your patients from the irrigants like sodium hypochlorite. We all know that bleach tastes awful, and rubber dams prevent that experience for our patients!
Drag to resize
Connecting Dentists with Quality, Interactive Dental Training
Has this closer evaluation affected your stance on rubber dam usage in dentistry? Whether you're choosing to practice with rubber dams or are still unsure about finding the perfect tool to isolate dentistry in your practice, my hope is that you now know you are not alone in trying to perfect and protect during treatment.
My goal is to promote information that provokes authentic, comprehensive, continuous, creative, and challenging learning experiences, and invite others to give their feedback.
If you feel strongly about dental dams or its alternatives, join our community and participate in the discussion.
My goal is to promote information that provokes authentic, comprehensive, continuous, creative, and challenging learning experiences, and invite others to give their feedback.
If you feel strongly about dental dams or its alternatives, join our community and participate in the discussion.
Drag to resize
Drag to resize
Related courses:
Dennis Hartlieb, DDS, AAACD
DOT Founder
Share this page
Join 10,000+ dentists who get tips bi-weekly.
Thank you!
By signing up you agree to our Privacy Policy.
Latest from our blog

Our vision is to provide online continuing education workshops and mentorship that are comprehensive for dentists learning at all career levels. DOT is developed for dentists that love to learn online.
CONNECT
Materials Included
Light Brown tints, Enamelize, Unfilled Resin Flexidiscs, Flexibuffs 1/2", #1 artist’s brush, Silicone Polishing Points, IPC Off Angle Short Titanium Coated Composite Instrument
Materials Needed, not Included
- Loupes
Follow along
You are Registered
We’re excited to have you join us! You’ll receive email reminders at with the link to join this event.
If you have any questions in the meantime, feel free to reach out to us at dot@dothandson.com—we’re here to help!
Day 1 (8 - 4 pm CST)
-
Erosion and wear – the why and the how
-
Adding length to teeth – when is it safe
-
Opening VDO to compensate for lost tooth structure – where to begin
-
Records visit and key points you need to understand before you start
-
The smile – the 7 strategic points to consider when evaluating the smile
-
Anterior tooth shape, morphology
-
Clinical case review
-
Upper Putty matrix construction
-
Build lingual incisal wall with putty matrix #6 - #11/ Upper anteriors
-
Full contour build-up #6, #7, #8, #9, #10, #11, shape and polish/ Upper anteriors
Day 2 (8 - 2 pm CST)
-
Who – which patients are candidates
-
Why – explaining to patients the value of the prototype
-
How – step-by-step techniques to maximize predictability, efficiency and success
-
Getting to Yes: conversations with patients about esthetic and reconstructive dentistry
-
The ‘Smile Preview’ – techniques to show the possibilities
-
Lower Putty matrix construction
-
Build lingual incisal wall with putty matrix #22 - #27 / lower anteriors
-
Build-up #22 - #27, shape and polish / lower anteriors
-
Build-up lower occlusal posteriors
-
Demonstration of Smile Preview
Upcoming Virtual Workshops
Write your awesome label here.
December 11 & 12, 2025
CPR for the Worn Dentition (16 CE)
Write your awesome label here.
January 29-30, 2026
Porcelain Veneer Cementation Workshop (14 CE)
Write your awesome label here.
March 27, 2026
Esthetic and Functional Success for Diastema Closure (8 CE)
Write your awesome label here.
May 15, 2026
From Break to Beautiful: Flawless Class IV Resin Restorations (8 CE)
Write your awesome label here.
June 19, 2026
Mastering Intraoral Scanners and Digital Workflow for the Dental Team (4 CE)
Write your awesome label here.
September 25, 2026
Veneering the Dark Central Incisor - Conservative Direct and Indirect Restorative Strategies (8 CE)
Write your awesome label here.
October 30, 2026
3D Printing for the Restorative Dentist
Write your awesome label here.
December 11, 2026
Injection Molding Workshop (8 CE)
Write your awesome label here.
Study Club
Join five in-depth virtual meetings held on Thursday evenings throughout the year. Engage in detailed case presentations, discuss curated research articles, and exchange valuable tips with fellow dentists.
-
01/22/2026
-
04/09/2026
-
06/11/2026
-
10/15/2026
-
12/10/2026
Write your awesome label here.
Coffee & Donuts
Kickstart your Friday mornings with informal sessions and discuss patient treatments, practice management, and receive feedback on your cases.
-
01/16/2026
-
02/13/2026
-
03/20/2026
-
04/10/2026
-
05/08/2026
-
06/05/2026
-
08/21/2026
-
10/09/2026
-
11/20/2026
-
12/10/2026
Popular On-Demand Courses
Write your awesome label here.
Injection Moulding Techniques (3 CE)
Simple, predictable, systematic foundation for you to start your journey with injection moulding
Write your awesome label here.
Advanced Techniques in Composite Veneers (6 CE)
Take control of aesthetic cases in your practice, whether you are enhancing smiles with direct resin veneers or creating provisional restorations for indirect cases.
Write your awesome label here.
A Realistic Perspective on Occlusal Appliances (3 CE)
Learn how to design, fabricate, and manage occlusal appliances with confidence through practical guidance and real clinical case examples.
Write your awesome label here.
Bicuspid Veneer and V-Onlay Preparation (3 CE)
Gain expertise in ‘prep-less’ veneers, buccal cusp reduction, and margin placement methods to enhance your clinical outcomes.
Write your awesome label here.
Class IV Composite Restoration – Polychromatic Approach (3 CE)
This on-demand course covers material selection and advanced layering techniques to help you create natural-looking, long-lasting restorations that set you apart.
Write your awesome label here.
EXOCAD: Foundation (2 CE)
Gain the skills to confidently navigate Exocad, build patient cases, and streamline your workflow using time-saving techniques and presets.
Write your awesome label here.
Class II Direct Resin (3 CE)
Master a reliable approach to Class II restorations by learning how to create ideal proximal contacts that enhance both the strength and aesthetics of your work.